General principle of chemotherapy Category
swaraj barik
#poet #writer I live with pride and self-respect.Writing is not my profession but my addiction . Medical Consultant,NursingStaff onlinemedical tutor
Brief information about general principle of chemotherapy
 Edumat.in
Edumat.in


General Principles of Chemotherapy
What is Chemotherapy?
Derived from "Chemo" (Chemical) and "Therapy" (Treatment).
It refers to the use of chemical agents to destroy disease-causing microorganisms or target cancerous cells selectively.
Antimicrobial Agents
1. Antibiotics
Naturally produced by microorganisms to inhibit or kill other microbes at low concentrations.
2. Chemotherapeutic Agents
Can be synthetic, semi-synthetic, or natural compounds that eliminate pathogens while causing minimal harm to the host.
3. Anti-Microbial Agents
Combination of chemotherapeutic agents and antibiotics that selectively act against microbial infections.
History of Chemotherapy
Paul Ehrlich (1908) – Father of Chemotherapy (Developed Arsphenamine).
Alexander Fleming (1928) – Discovered Penicillin.
Gerhard Domagk (1932) – Developed Sulfonamides.
Principles of Antimicrobial Therapy
1. Accurate Diagnosis
Identify site of infection.
Determine causative microorganism.
Select effective antimicrobial agents.
2. Necessity of Chemotherapy
Acute infections → Require chemotherapy.
Chronic infections → May need surgical intervention.
3. Drug Selection Criteria
Antimicrobial activity.
Pharmacokinetics (Absorption, distribution, metabolism, excretion).
Patient factors (Allergy, renal function, immune status).
4. Dosage & Duration
Use optimized doses to prevent resistance.
Inadequate dosing → Leads to drug resistance.
5. Continuous Therapy
Some infections resolve in 5–10 days, while others require prolonged treatment:
Typhoid Fever
Tuberculosis
Infective Endocarditis
6. Prophylactic Chemotherapy
Used before surgery to prevent infections.
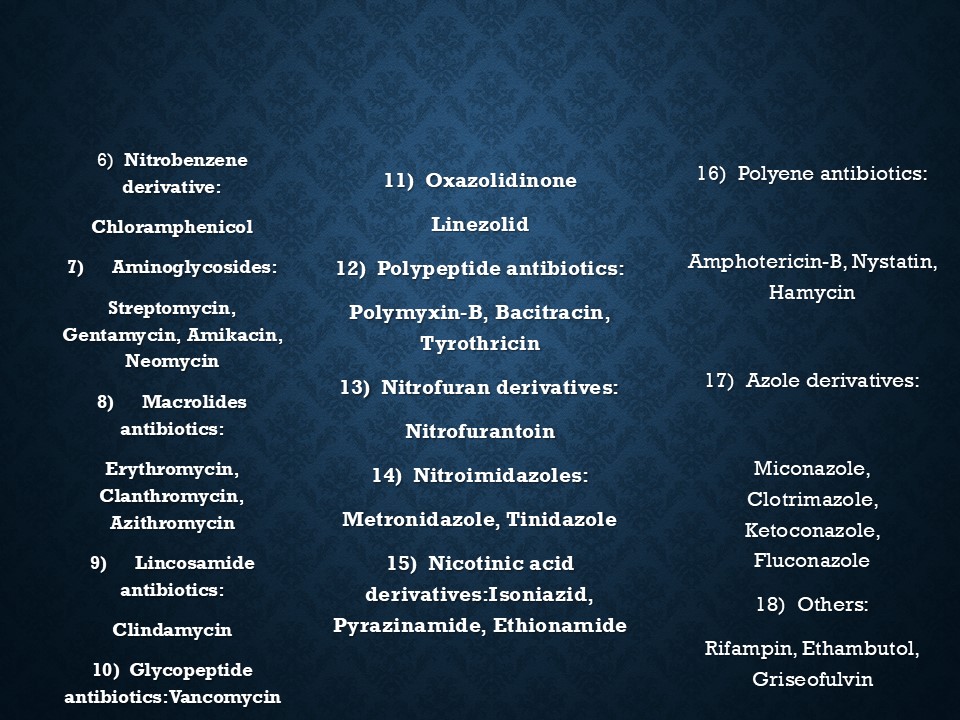
Classification of Antimicrobial Agents
A. Based on Chemical Structure
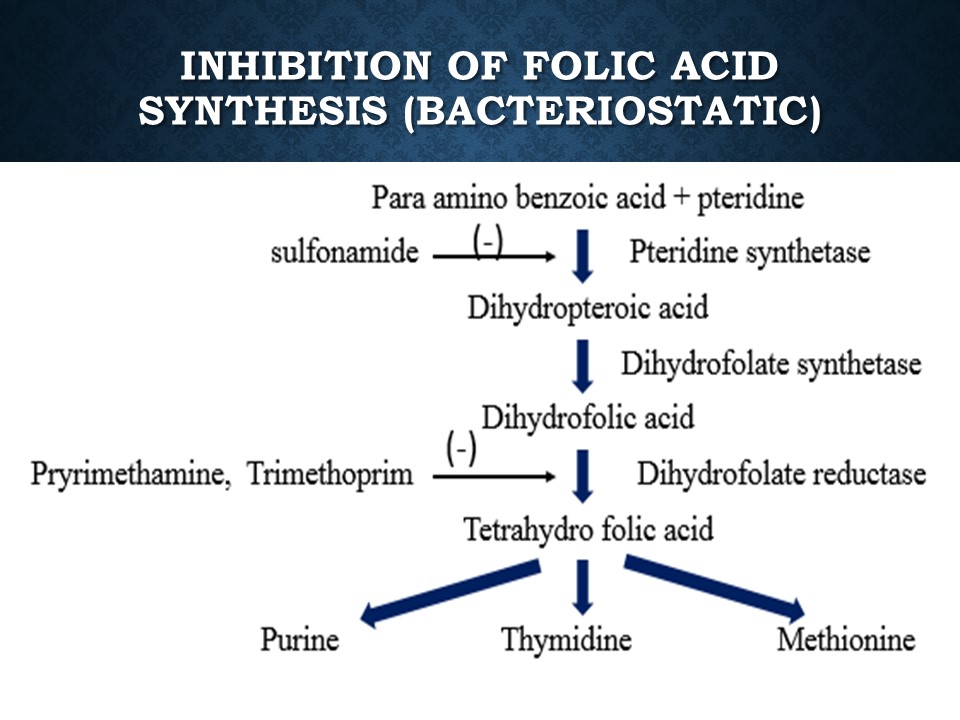
1. Sulfonamides & Related Drugs → Dapsone, Sulfadiazine
2. Diaminopyrimidines → Trimethoprim, Pyrimethamine
3. Quinolones → Nalidixic acid, Ciprofloxacin
4. Beta-Lactams → Penicillins, Cephalosporins
5. Tetracyclines → Doxycycline, Oxytetracycline
6. Aminoglycosides → Streptomycin, Gentamicin, Amikacin
7. Macrolides → Erythromycin, Azithromycin
8. Glycopeptides → Vancomycin
9. Oxazolidinones → Linezolid
10. Nitroimidazoles → Metronidazole, Tinidazole
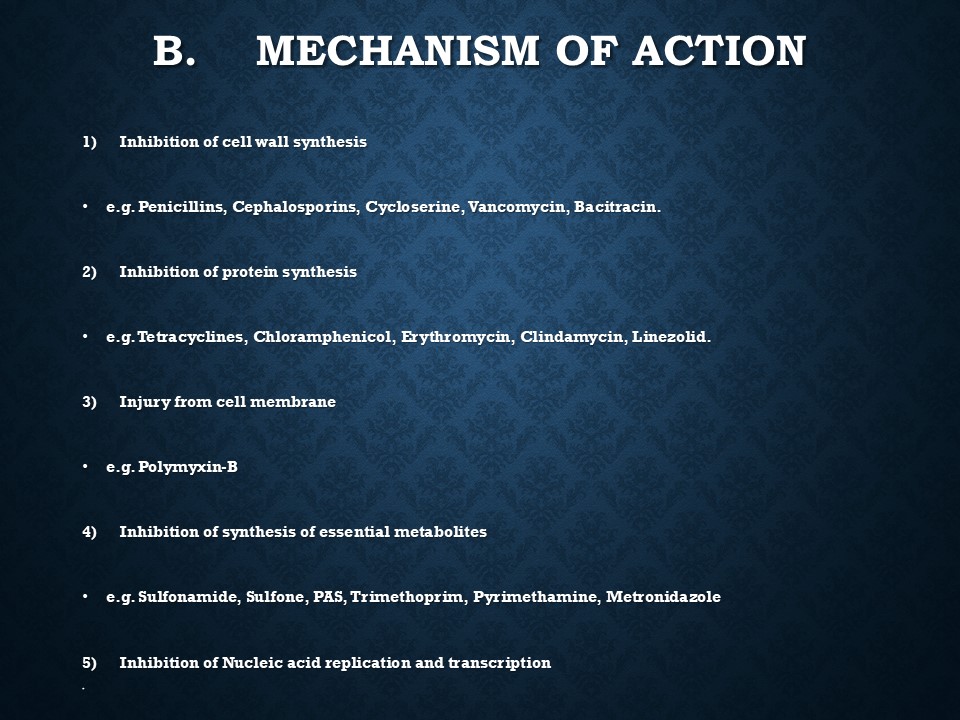
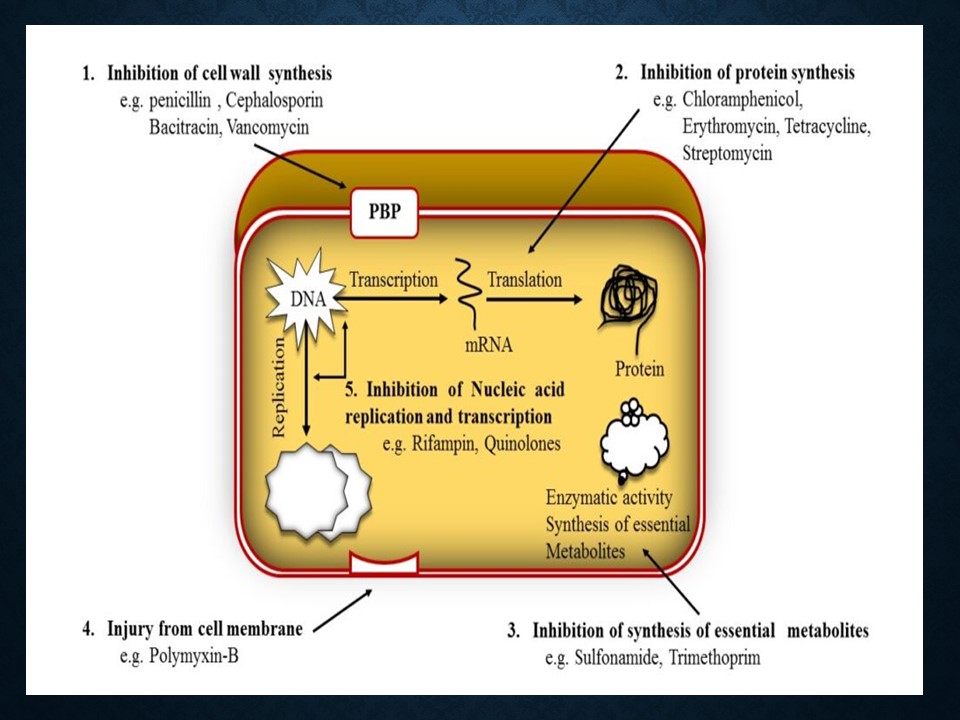
B. Based on Mechanism of Action
1. Inhibits Cell Wall Synthesis → Penicillins, Cephalosporins, Vancomycin
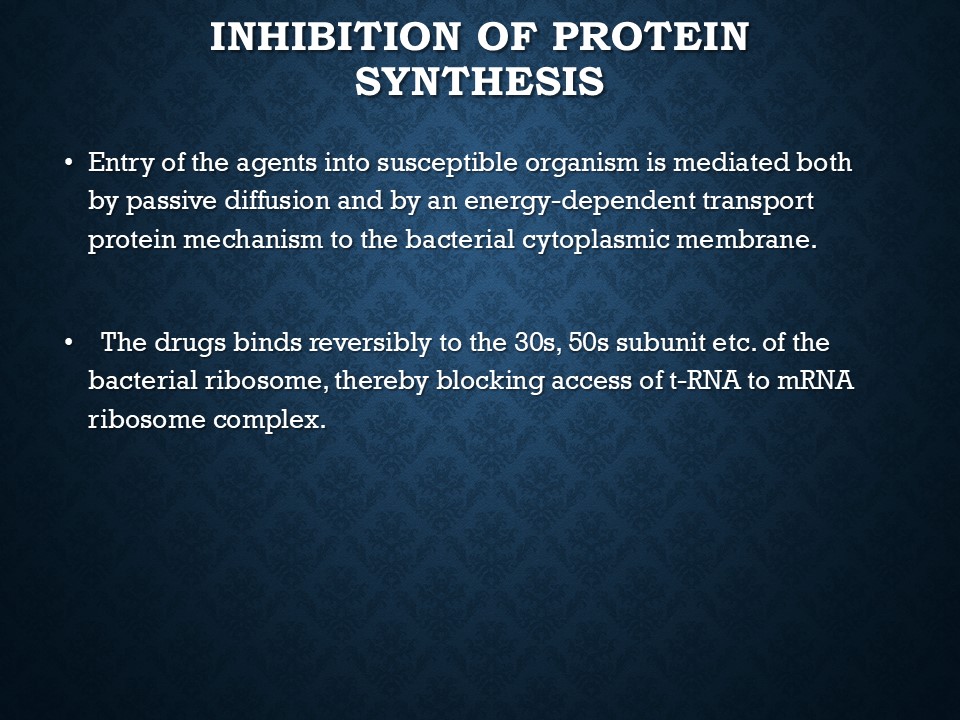
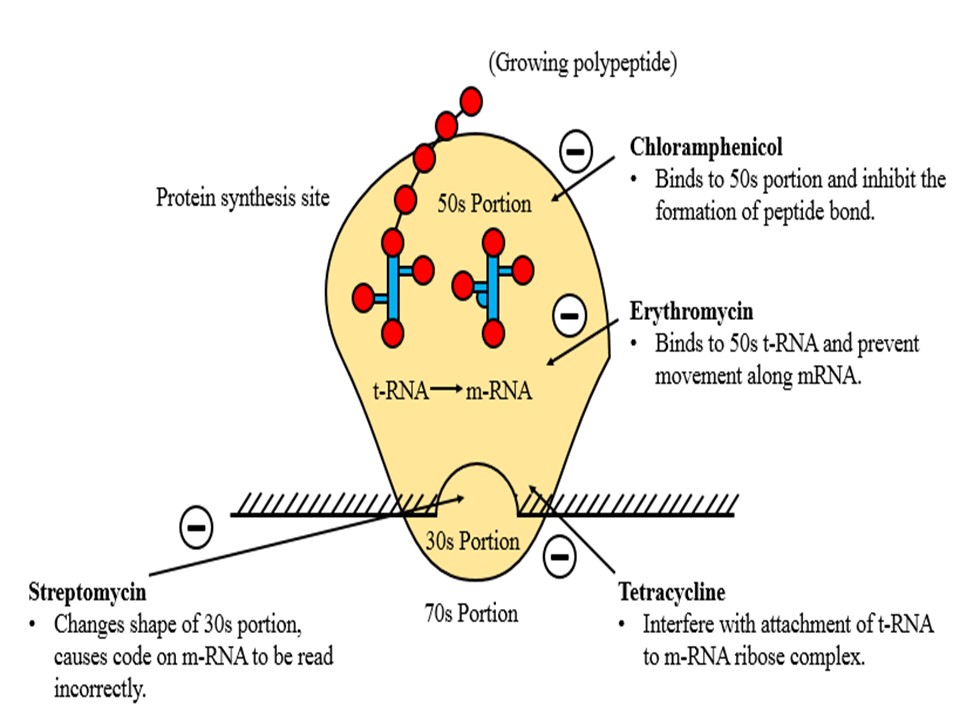
2. Inhibits Protein Synthesis → Tetracyclines, Macrolides, Aminoglycosides
3. Disrupts Cell Membrane → Polymyxins
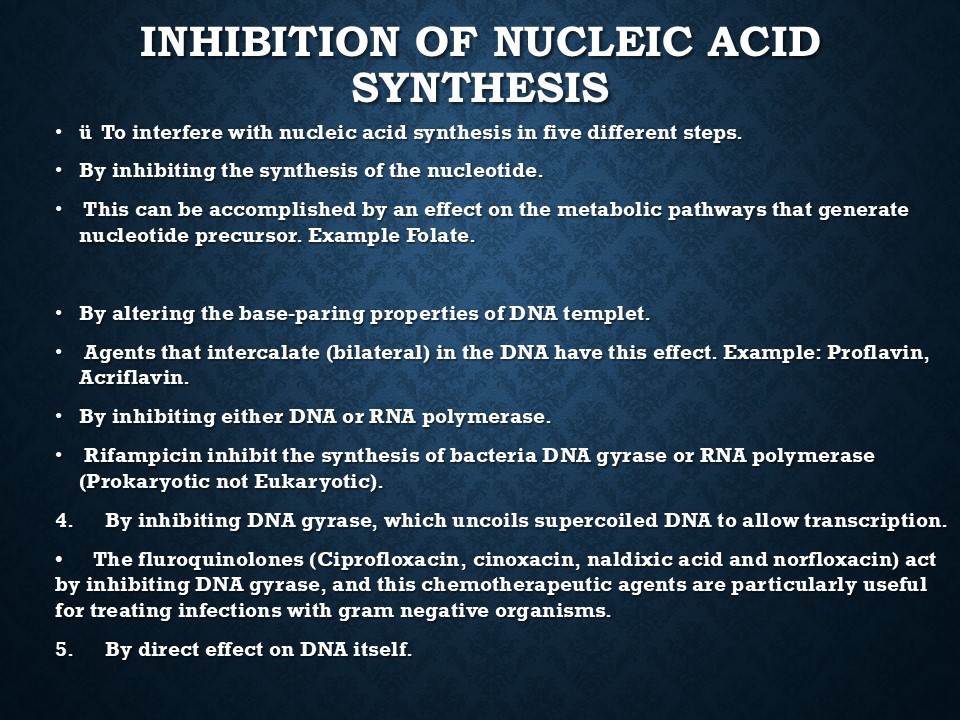
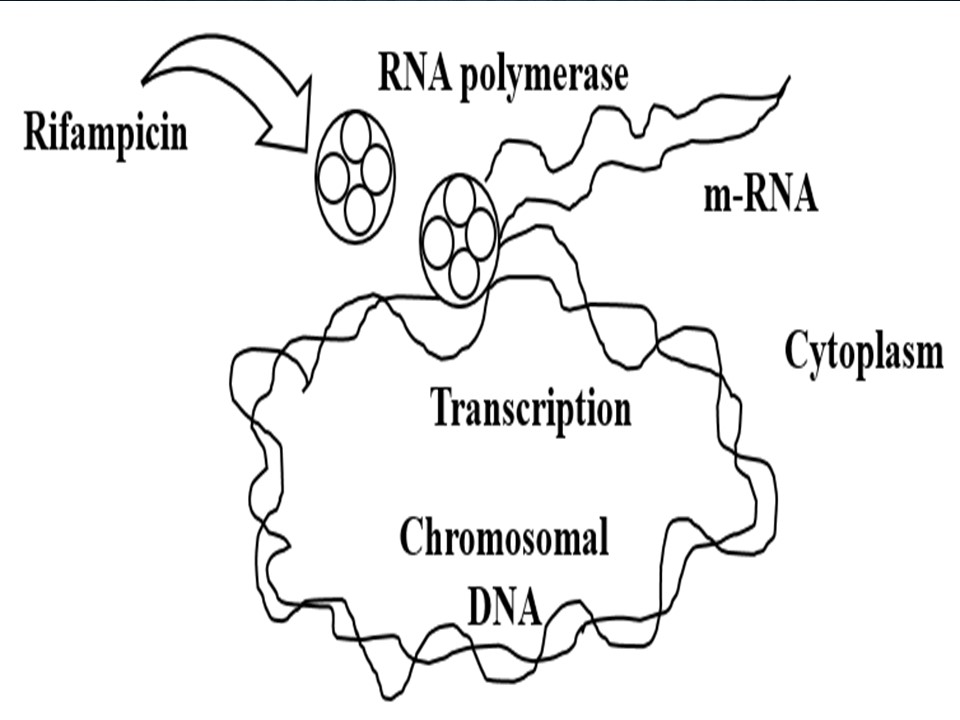
4. Inhibits DNA/RNA Synthesis → Rifampin, Quinolones
5. Blocks Essential Metabolites → Sulfonamides, Trimethoprim
C. Based on Target Organisms
Antibacterial → Penicillin, Erythromycin
Antiviral → Acyclovir, Zidovudine
Antifungal → Griseofulvin, Amphotericin B
Antiprotozoal → Metronidazole, Chloroquine
Antihelmintic → Mebendazole, Niclosamide
D. Based on Spectrum of Activity
Narrow Spectrum → Penicillin G, Streptomycin
Broad Spectrum → Tetracycline, Chloramphenicol
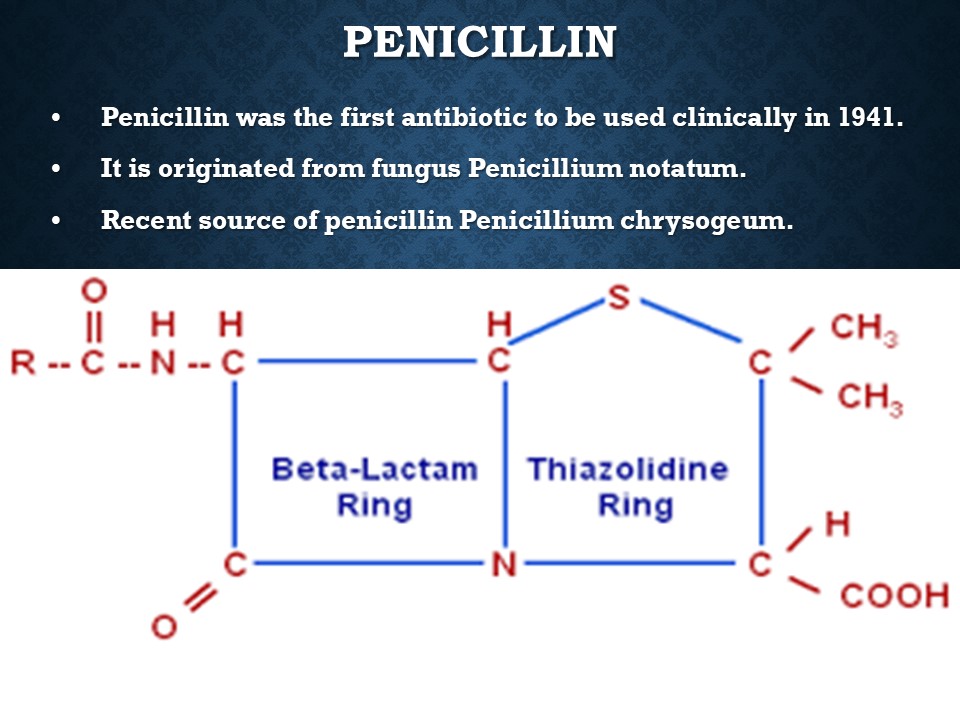
Penicillin: A Breakthrough Antibiotic
Discovered by: Alexander Fleming (1928)
Source: Penicillium notatum & Penicillium chrysogeum
First clinical use: 1941
Classification of Penicillins
1. Penicillin G Variants (Acid-sensitive)
Benzylpenicillin (Penicillin G)
Phenoxymethyl penicillin (Penicillin V) (Acid-resistant alternative to Pen G)
2. Penicillinase-Resistant Penicillins
Methicillin, Cloxacillin, Dicloxacillin
3. Extended-Spectrum Penicillins
Ampicillin, Amoxicillin, Piperacillin
4. Beta-Lactamase Inhibitors (Enhance Penicillin Activity)
Clavulanic Acid, Sulbactam, Tazobaco
Mechanism of Action of Penicillin
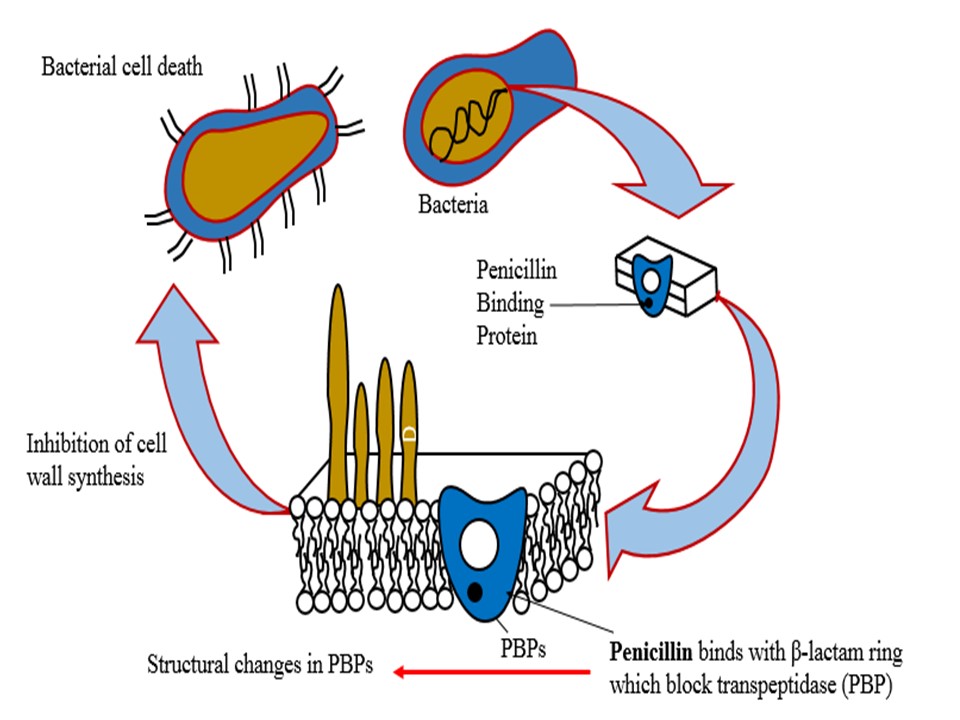
1. Inhibits Cell Wall Synthesis
Binds to Penicillin-Binding Proteins (PBPs) → Prevents cross-linking → Bacterial cell lysis.
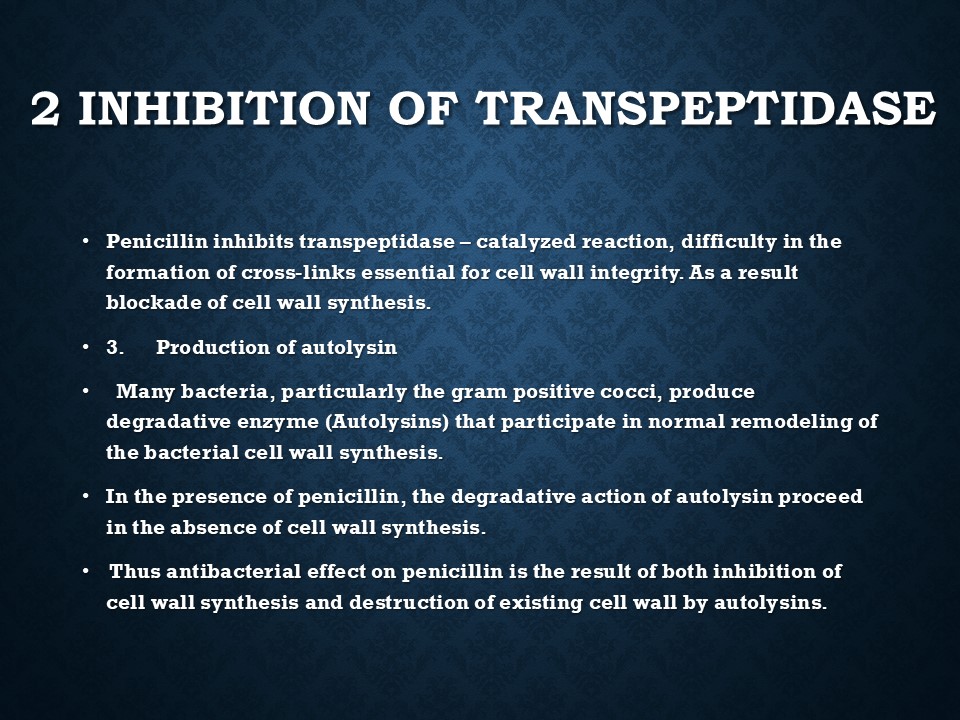
2. Inhibits Transpeptidase
Prevents peptidoglycan cross-linking, weakening the cell wall.
3. Activates Autolysins
Induces self-destruction of bacterial cell walls.
Resistance to Penicillin
1. Enzyme-Mediated Resistance
Penicillinase (β-lactamase) inactivates Penicillin G.
Found in Staphylococci, E. coli, H. influenzae.
2. Target Modification
Altered PBPs reduce penicillin binding → Common in MRSA (Methicillin-Resistant Staphylococcus Aureus).
3. Decreased Permeability
Gram-negative bacteria have outer membranes, preventing penicillin entry.
Pharmacokinetics of Penicillin G
Acid-labile (Destroyed by gastric acid).
Rapid absorption (IM route preferred).
Short half-life (~30 min in adults).
Does not cross BBB easily (Except in meningitis).
Excreted via kidneys (Renal impairment affects clearance).
Adverse Effects of Penicillin
1. Local & Systemic Toxicity
Pain at injection site (IM)
Thrombophlebitis (IV)
Neurotoxicity (High doses → Confusion, seizures)
2. Hypersensitivity Reactions
Mild: Rash, itching, fever.
Severe: Anaphylaxis, Angioedema.
3. Jarisch–Herxheimer Reaction
Occurs in syphilis treatment → Fever, muscle pain, vascular collapse.
Therapeutic Uses of Penicillin
A. Bacterial Infections
Streptococcal Infections → Pharyngitis, Rheumatic fever
Pneumococcal Infections → Pneumonia, Meningitis
Meningococcal Meningitis
Syphilis (Drug of Choice)
Diphtheria, Tetanus, Anthrax
B. Prophylactic Uses
Rheumatic fever prevention
Bacterial endocarditis prevention
Recommended

Adverse Drug Reaction (ADR)
31 slides • 5 months ago
Ball Mill principle
10 slides • 5 months ago
Important questions of BSC nursing final year exam
12 slides • 5 months ago
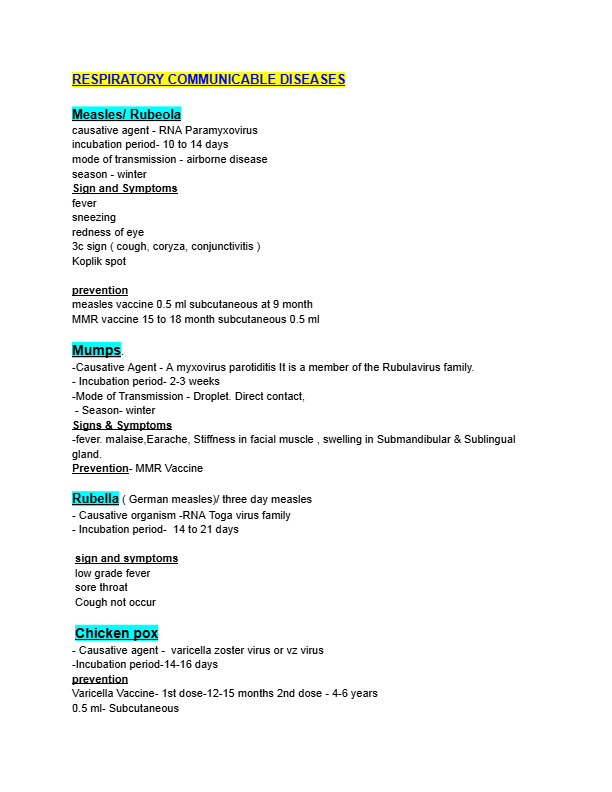
RESPIRATORY COMMUNICABLE DISEASES
5 slides • 4 months ago